
NATIONAL HEALTH INSURANCE IN SOUTH AFRICA
POLICY PAPER
1. INTRODUCTION
1. South Africa is in the process of introducing an innovative system of healthcare financing with far reaching consequences on the health of South Africans. The National Health Insurance commonly referred to as NHI will ensure that everyone has access to appropriate, efficient and quality health services. It will be phased-in over a period of 14 years. This will entail major changes in the service delivery structures, administrative and management systems.
2. The NHI is intended to bring about reform that will improve service provision. It will promote equity and efficiency so as to ensure that all South Africans have access to affordable, quality healthcare services regardless of their socio-economic status.
3. The current system of healthcare financing in South Africa is two-tiered, with a relatively large proportion of funding allocated through medical schemes, various hospital care plans and out of pocket payments. This current funding arrangement provides cover to private patients who have purchased a benefit option with a scheme of their choice or as a result of their employment conditions. It only benefits those who are employed and are subsidised by their employers - both the State and the private sector. The other portion is funded through the fiscus and is mainly for public sector users. This means that those with medical scheme cover have a choice of providers operating in the private sector which is not extended to the rest of the population.
4. A larger part of the financial and human resources for health is located in the private health sector serving a minority of the population. Medical schemes are the major purchasers of services in the private sector which covers 16.2% of the population (CMS1, 2009). The public sector is under-resourced relative to the size of the population that it serves and the burden of disease. The public sector has disproportionately less human resources than the private sector yet it has to manage significantly higher patient numbers.
5. The South African health system is inequitable, with the privileged few having disproportionate access to health services. There is recognition that this system is neither rational nor fair. Therefore, NHI is intended to ensure that all South African citizens and legal residents will benefit from healthcare financing on an equitable and sustainable basis. NHI will provide coverage to the whole population and minimise the burden carried by individuals of paying directly out of pocket for healthcare services. This model of delivering health and healthcare services to the population is well accepted, described and widely promoted by the World Health Organisation as universal coverage.
6. To successfully implement a healthcare financing mechanism that covers the whole population such as NHI, four key interventions need to happen simultaneously: i) a complete transformation of healthcare service provision and delivery; ii) the total overhaul of the entire healthcare system iii) the radical change of administration and management iv) the provision of a comprehensive package of care underpinned by a re-engineered Primary Health Care.
2. PROBLEM STATEMENT
7. Prior to the 1994 democratic breakthrough, South Africa had a fragmented health system designed along racial lines. One system was highly resourced and benefitted the white minority. The other was systematically under-resourced and was for the black majority. The Constitution has outlawed any form of racial discrimination and guarantees the principles of socioeconomic rights including the right to health.
8. Attempts to deal with these disparities and to integrate the fragmented services that resulted from fourteen health departments (serving the four race groups, including the ten Bantustans) did not fully address the inequities. Problems linked to health financing that are biased towards the privileged few have not been adequately addressed.
9. Post 1994 attempts to transform the healthcare system and introduce healthcare financing reforms were thwarted. This has entrenched a two-tiered health system, public and private, based on socioeconomic status and it continues to perpetuate inequalities in the current health system. Attempts to reform the health system have not gone far enough to extend coverage to bring about equity in healthcare.
10. The two-tiered system of healthcare did not and still does not embrace the principles of equity and access and the current health financing mode does not facilitate the attainment of these noble goals.
11. The 2008 World Health Report of the World Health Organisation (WHO) details three trends that undermine the improvement of health outcomes globally, namely:
- Hospital centrism, which has a strong curative focus
- Fragmentation in approach which may be related to programmes or service delivery, and
- Uncontrolled commercialism2 which undermines principles of health as a public good
12. An analogy of the preceding description can be drawn with the negative attributes of the South African two-tier healthcare system, which are unsustainable, destructive, very costly and highly curative or hospi-centric3.
13. The national health system has a myriad of challenges, among these being the worsening quadruple4 burden of disease and shortage of key human resources. The public sector has underperforming institutions that have been attributed to poor management, underfunding, and deteriorating infrastructure.
14. In many areas access has increased in the public sector, but the quality of healthcare services has deteriorated or remained poor. The public health sector will have to be significantly changed so as to shed the image of poor quality services that have been scientifically shown to be a major barrier to access (Bennett & Gilson, 2003).
15. Similarly to the public health system, the private sector also has its own problems albeit these are of a different nature and mainly relate to the costs of services. This relates to the pricing and utilisation of services. The high costs are linked to high service tariffs, provider-induced utilization of services and the continued over-servicing of patients on a fee-for-service basis. Evidently, the private health sector will not be sustainable over the medium to long term.
16. To change these types of systems will require transformation of the healthcare financing model, better regulation of healthcare pricing, improvement in quality of healthcare as well as the strengthening of the planning, information management, service provision and the overhauling of management systems.
2.1 THE BURDEN OF DISEASE IN SOUTH AFRICA
17. The introduction of NHI, should take into account the burden of disease the country is experiencing. South Africa is plagued by four clear health problems that have been described in the Lancet Report as the quadruple burden of disease (Coovadia et al, 2009). These are:
- HIV/AIDS and TB
- Maternal, infant and child mortality
- Non-communicable diseases
- Injury and violence
2.1.1 HIV/AIDS and TB
18. Despite South Africa only having 0.7% of the world population it carries 17% of HIV infected people in the world. The HIV prevalence is twenty three times the global average, while the TB infection rate is among the highest in the world. Moreover, the TB and HIV/AIDS co-infection rate is one of the highest in the world at 73%. As a result life expectancy in South Africa has declined over a number of years. HIV/AIDS has also contributed significantly to high maternal and child mortality rates. Failure to intervene may reverse 50 years of health gains.
2.1.2 Maternal, Child and Infant Mortality
19. The maternal mortality ratios5, peri-natal mortality6 and neonatal mortality7 rates in South Africa are much higher than that of countries of similar socio-economic development. Maternal mortality has increased markedly in our country, and as previously mentioned HIV/AIDS is the main contributor. However, there are also deaths that are due to largely preventable and non-AIDS related factors. Similarly, infant and child mortality rates have reached unacceptably high levels not only due to HIV and AIDS but also due to other preventable causes.
2.1.3 Non-Communicable Diseases
20. Non-communicable diseases such as high blood pressure, diabetes, chronic heart disease, chronic lung diseases, cancer and mental illnesses contributed to 28% of the total burden of disease measured by disability-adjusted life years in 2004. They are largely driven by four risk factors, namely alcohol, smoking, poor diet, and lack of exercise.
2.1.4 Injury and Violence
21. Injury and violence are also contributing significantly to the burden of disease. Injuries may be categorised as either intentional or unintentional. Of note is the significant proportion of injury associated with road accidents and inter-personal violence, particularly, violence against women and children. These are driven largely by high alcohol consumption and other social factors such as poverty and unemployment.
2.2 QUALITY OF HEALTHCARE
22. As mentioned earlier, significant improvements in health services coverage and access since 1994 have been achieved. However, there are still notable quality problems. Among the commonly cited and experienced by the public are: cleanliness, safety and security of staff and patients, long waiting times, staff attitudes, infection control and drug stock-outs.
23. Given that there are concerns about quality at public sector facilities, there is preference by the public for services in the private sector which may largely be funded out of pocket. Various members of the public cannot afford to make these payments. This type of arrangement is not suitable for the country‟s level of development. Therefore, improvement of quality in the public health system is at the centre of the health sector‟s reform endeavours.
2.3 HEALTHCARE EXPENDITURE IN SOUTH AFRICA
24. The World Health Organisation recommends that countries spend at least 5% of their GDP on health care. South Africa already spends 8.5% of its GDP on health, way above what WHO recommends. Despite this high expenditure the health outcomes remain poor when compared to similar middle-income countries. This poor performance has been attributed mainly to the inequities between the public and private sector.
25. It has been reported that high-income countries spent an average of 7.7 percent of their GDP (Gross Domestic Product)8 on health whilst middle income countries spent 5.8 percent, and low income countries spent 4.7 percent (Schieber, et al 2006).
26. The 8.3% of GDP spent on health is split as 4.1% in the private sector and 4.2 % in the public sector. The 4.1% spend covers 16.2 % of the population, (8.2 million people) who are largely on medical schemes. The remaining 4.2% is spent on 84% of the population
(42 million people) who mainly utilize the public healthcare sector (National Treasury: Intergovernmental Fiscal Review, 2011).
27. Over the past decade, private hospital costs have increased by 121% whilst over the same period, specialist costs have increased by 120% (CMS Report, 2008). This means that the private healthcare sector will have to accept that the charging of exorbitant fees completely out of proportion to the services provided have to be radically transformed. In real terms, contribution rates per medical scheme beneficiary have doubled over a seven-year period. This has not been proportionate with increased access to services. Simply put this has meant limited access to needed health service coverage mainly as a result of the design of the medical scheme benefit options, or due to early exhaustion of benefits.
28. In South Africa health care expenditure is derived from three main sources: public sector expenditures financed out of general revenue, private sector expenditures financed through medical schemes, and out of pocket payments. This is consistent with expenditure trends as reported by the World Bank (World Bank 2004).
2.4 DISTRIBUTION OF FINANCIAL AND HUMAN RESOURCES
29. The mal-distribution of healthcare resources described above leads to a skewed distribution of key healthcare professionals in favour of the private sector.
30. The recent estimates show that the ratio of patients to health professionals (specialists, general practitioners, pharmacists) is lower in the private sector than in the public sector. There are more professionals per patient in the private sector than the public sector. The Department is finalising its human resources for health strategy in order to the shortages in human resources.
31. The amount spent in the private health sector relative to the total number of people covered is not justifiable and defeats the principles of social justice and equity. Per capita annual expenditure for the medical aid group has been estimated at R11,150.00 in contrast to public sector dependant population where the per capita annual health expenditure is estimated at R2,766.00. This is not an efficient way of financing healthcare.
2.5 MEDICAL SCHEMES INDUSTRY
32. Presently the most reliable source of healthcare financing for individuals is in the form of medical schemes and various hospital cash plans. However, over the years many of them have experienced problems of sustainability. A number of medical schemes have collapsed, been placed under curatorship or merged. They have reduced from over 180 in the year 2001 to about 102 in 2009. This was mainly due to over pricing of health care.
33. In a bid to sustain their financial viability, many schemes resorted to increasing premiums, in many cases at rates higher than CPIX. When this was not successful, the schemes resorted to decreasing members benefits. This has led to an increasing number of members exhausting their benefits midyear or towards the end of the year. This has been worsened by non-health related exorbitant administrator's fees, oversupply of brokers, disproportionate to the membership, and managed care costs. As a result, increased deductions of medical scheme contribution from member's salaries have resulted in wage inflation.
34. However, it is evident that the above measures did not improve or have worsened the cost-escalation because at the centre of this problem is the uncontrolled commercialism of healthcare as described by the World Health Organisation. The intervention by the Competition Commission was also clearly based on the understanding that the scenario is as mapped above. Clearly something completely different is needed in the South African health sector.
2.6 OUT OF POCKET PAYMENTS AND CO-PAYMENTS
35. Out of pocket payment accounts for a significant part of total health expenditure and this could be in the form of co-payments, or direct payment to private providers particularly by those who are not covered by medical schemes. Even for those who are covered by medical schemes, the extent of co-payments confirms that the current system does not provide full cover. However, for those who are not on medical aid this could have catastrophic9 effects.
36. Payment for health care, particularly for those who cannot afford and who pay out of pocket cannot be planned in advance and this lack of predictability is what exposes households to financial hardships.
37. Evidence has demonstrated that those who are not adequately covered by any form of health insurance are among others women; children; the elderly; low income groups etc. It is for this reason that coverage should be extended to all these populations (Meng, 2011).
3. HISTORY OF PROPOSALS ON HEALTHCARE FINANCING REFORM IN SOUTH AFRICA
38. Contrary to common belief, the history of reforming the healthcare financing system in South Africa actually dates back more than 80 years:
3.1 Commission on Old Age Pension and National Insurance (1928)
39. A Commission on Old Age Pension and National Insurance recommended that a health insurance scheme should be established to cover medical, maternity and funeral benefits for all low income formal sector employees in urban areas.
3.2 Committee of Enquiry into National Health Insurance (1935)
40. A Committee of Enquiry into National Health Insurance recommended in 1935 similar proposals as those made in 1928. Neither of the proposals of these two Committees was ever taken forward.
3.3 National Health Service Commission (1942 - 1944)
41. A Commission led by Dr. Henry Gluckman was set up in this period. It was called the National Health Service Commission. It recommended the implementation of a National Health Tax to ensure that health services could be provided free at the point of service for all South Africans. The aim was to bring health services "within reach of all sections of the population, according to their needs, and without regard to race, colour, means or station in life". Health centres, providing comprehensive primary care services, were proposed as a core component of the health system.
42. Although the Gluckman Commission proposals were accepted by the government led by General Jan Smuts, it was decided to implement them as a series of measures rather than in a single step. The introduction of Community-based centres was taken forward with 44 centres being in operation within two years, but other aspects of the proposals were never implemented. Any gains from the Gluckman Commission process were reversed after the National Party (NP) government led by General DF Malan was elected in 1948.
3.4 Health Care Finance Committee (1994)
43. By the early 1990s, the spotlight had again turned to the possibility of introducing some form of mandatory health insurance and after the 1994 elections; there were several policy initiatives that considered either social or national health insurance. The Healthcare Finance Committee of 1994 recommended that all formally employed individuals and their immediate dependents should initially form the core membership of social health insurance arrangements with a view to expanding coverage to other groups over time.
44. It was also suggested that there should be a multi-funder (or multi-payer) environment and that private funders, namely medical schemes, should act as financial intermediaries for channelling funds to providers. It was also proposed that there should be a risk-equalization10 mechanism between individual insurers to help stabilise the medical schemes industry. It was further recommended that a comprehensive set of services be covered under such a system and that both public and private providers will be involved in the delivery and provision of these services. The main challenge with respect to these sets of recommendations was the inability of the State to fully finance the recommended package of services.
3.5 Committee of Inquiry on National Health Insurance (1995)
45. The 1994 Finance Committee was followed by the 1995 Commission of Enquiry on National Health Insurance which fully supported the recommendations of the Health Finance Committee. The key difference was on the benefit package. This committee as well as the healthcare finance committee made a strong case for primary health care services.
3.6 The Social Health Insurance Working Group (1997)
46. In 1997 the Social Health Insurance Working Group developed the regulatory framework that resulted in the enactment of the Medical Schemes Act in 1998. This Act was meant to regulate the private health insurance as well as to entrench the principles of open enrolment, community rating, prescribed minimum benefits and better governance of medical schemes. However, despite the introduction of the Act and the supporting principles the level of coverage for the national population has remained below 16 percent and is only affordable to the relatively well-off.
3.7 Committee of Inquiry into a Comprehensive Social Security for South Africa (2002)
47. In 2002, Department of Social Development appointed Professor Vivienne Taylor to chair the Committee of Inquiry into a Comprehensive Social Security for South Africa. The Commission recommended that there must be mandatory cover for all those in the formal sector earning above a given tax threshold and that contributions should be income-related and collected as a dedicated tax for health. The Committee also recommended that the State should create a national health fund through which resources should be channelled to public facilities through the government budget processes.
3.8 Ministerial Task Team on Social Health Insurance (2002)
48. To implement the recommendations of the Taylor Committee, the Department of Health established the Ministerial Task Team on Social Health Insurance in 2002 to draft an implementation plan with concrete proposals on how to move towards social health insurance and to create supporting legislative and institutional mechanisms that will in the long term result in the realisation of National Health Insurance in South Africa. However, the path to achieving universal coverage through a social health insurance model was not widely supported and the implementation of the supporting proposals thus stalled.
3.9 Advisory Committee on National Health Insurance (2009)
49. In August 2009, the Ministerial Advisory Committee on National Health Insurance was established which had been tasked with providing the Minister of Health and the Department of Health with recommendations regarding the relevant health system reforms and matters relating to the design and roll-out of National Health Insurance. This was to carry forward the Resolution passed at the ruling party‟s (ANC) Conference in December 2007 in Polokwane. This was Resolution 53 which called for the establishment of a National Health Insurance.
4. NATIONAL HEALTH INSURANCE
50. The rationale for introducing National Health Insurance is therefore to eliminate the current tiered system where those with the greatest need have the least access and have poor health outcomes. National Health Insurance will improve access to quality healthcare services and provide financial risk protection against health-related catastrophic expenditures for the whole population. Such a system will provide a mechanism for improving cross-subsidization in the overall health system, whereby funding contributions would be linked to an individual's ability-to-pay and benefits from health services would be in line with an individual's need for care. Moreover, by significantly reducing direct costs for health care, families and households under National Health Insurance are less likely to face impoverishing health care costs.
51. NHI will ensure that everyone has access to a defined comprehensive package of healthcare services. The covered healthcare services will be provided through appropriately accredited and contracted public and private providers and there will be a strong and sustained focus on the provision of health promotion and prevention services at the community and household level.
5. PRINCIPLES OF NATIONAL HEALTH INSURANCE IN SOUTH AFRICA
52. The National Health Insurance will be guided by the following principles:
a) The Right to Access - Section 27 of the Bill of Rights of the Constitution states that everyone has a right of access to health care services including reproductive health care and that the State must take reasonable legislative and other measures, within its available resources, to achieve the progressive realisation of these rights. The reform of healthcare is an important step towards the realisation of these rights and the key aspect of this is that access to health services must be free at the point of use and that people will benefit according to their health profile.
b) Social Solidarity - this refers to the creation of financial risk protection for the entire population that ensures sufficient cross-subsidisation between the rich and the poor, and the healthy and sick. Such a system allows for the spreading of health costs over a person‟s lifecycle: paying contributions when one is young and healthy and drawing on them in the event of illness later in life.
c) Effectiveness - this will be achieved through evidence based interventions, strengthened management systems and better performance of the healthcare system that will contribute to positive health outcomes and overall improved life expectancy for the entire population.
d) Appropriateness - this refers to the adoption of new and innovative health service delivery models that take account of the local context and acceptability and tailored to respond to local needs. The health services delivery model will be based on a properly structured referral system rendered via a re-engineered Primary Health Care model.
e) Equity - this refers to the health system that ensures that those with the greatest health need are provided with timely access to health services. It should be free from any barriers11 and any inequalities in the system should be minimised. Equity in the health system should lead to expansion of access to quality health services by vulnerable groups and in underserved areas. The principle of equity has been elaborately articulated as fairness by the Director-General of the WHO, Dr. Margaret Chan (see box insert).
***
Dr. Margaret Chan Address to the United Nations General Assembly on the theme "Advancing Global Health in the Face of Crisis", 15 June 2009:
"Fairness, I believe, is at the heart of our ambitions in global health. A quest for greater fairness dominates the agenda for this forum. We see this in your concern about vulnerable populations, and about health systems that exclude the poor. We see this in your support for global health initiatives and funding mechanisms that redistribute some of the world's riches towards health needs of the poor. On the issue of fairness, let me again state the obvious. Our world is dangerously out of balance, also in matters of health. Differences, within and between countries, in income levels, opportunities and health status are greater today than at any time in recent history. Part of the world feasts itself into obesity, while part of the world fasts and starves for want of food. Part of the world thrives into old age, while part of the world dies young from easily and cheaply preventable causes. As the historians tell us, such huge extremes of privilege and misery are a precursor for social breakdown. Is this where the progress of our civilized, advanced, high-tech, sophisticated society has brought us? To the brink of social breakdown? Let me make another obvious point. A health system is a social institution. It does not just deliver pills and babies the way a post office delivers letters. Properly managed and financed, a health system that strives for universal coverage contributes to social cohesion and stability. I further believe that a failure to make fairness an explicit objective, in policies, in the systems that govern the way nations and their populations interact, is one reason why the world is in such a great big mess".
***
f) Affordability - this means that services will be procured at reasonable costs that recognise health as not just an ordinary commodity of trade but as a public good.
g) Efficiency - this will be ensured through creating administrative structures that minimize or eliminate duplication across the national, provincial and district spheres. The key will be to ensure that minimal resources are spent on the administrative structures of the National Health Insurance and that value-for-money is achieved in the translation of resources into actual health service delivery.
6. OBJECTIVES OF NATIONAL HEALTH INSURANCE
53. National Health Insurance is aimed at providing universal coverage. Universal coverage as defined by WHO "is the progressive development of a health system including its financing mechanisms into one that ensures that everyone has access to quality, needed health services and where everyone is accorded protection from financial hardships linked to accessing these health services".
54. A number of countries have reformed their health systems to achieve the above goals. This has brought about equity in access for needed services, administrative efficiency, increased revenue and quality improvements.
55. The objectives of National Health Insurance are:
a) To provide improved access to quality health services for all South Africans irrespective of whether they are employed or not.
b) To pool risks and funds so that equity and social solidarity will be achieved through the creation of a single fund.
c) To procure services on behalf of the entire population and efficiently mobilize and control key financial resources. This will obviate the weak purchasing power that has been demonstrated to have been a major limitation of some of the medical schemes resulting in spiralling costs.
d) To strengthen the under-resourced and strained public sector so as to improve health systems performance
7. SOCIOECONOMIC BENEFITS OF NATIONAL HEALTH INSURANCE
56. Health affects social development and economic productivity in four ways. These are namely through (i) increased output as a healthy person works more effectively and efficiently and devotes more time to productive activities (i.e. fewer days off, longer work life span); (ii) a broader knowledge base in the economy as the gains to education increase as life expectancy increases; (iii) increased "work life" and savings as a result of increased life expectancy may result in earning and saving more for retirement; and (iv) an increase in labour force activity. These benefits include having a healthier population, which in turn translates into a productive and effective workforce that grows local business, attracts foreign investors and grows the domestic economy.
57. This argument was effectively elaborated by the Secretary General of the United Nations, Mr. Ban Ki Moon, at the 2009 United Nations General Assembly on the theme "Advancing Global Health in the Face of Crisis", when he said:
"We can cut back on health expenditures and incur massive losses in lives and fundamental capacity for growth. Or we can invest in health and spare both people and economies the high cost of inaction. The cost of cutting back is just unthinkable. I know that many in this audience do not need to be told about the significant returns we see from investing in health. Investments to scale up basic health services can bring a six-fold economic return. Healthy people have improved life expectancy, go to school, are more productive, take fewer days off of work, have lower birth rates and thus invest more in fewer children".
58. In other middle-income countries where National Health Insurance has been implemented it has resulted in the following benefits:
a) A healthier population contributes to better wealth creation. Each extra year of life expectancy raises a country‟s GDP per person by around 4% in the long run. Poor health reductions in adult mortality explain 10 to 15 percent of the economic growth that occurred from 1960 to 1990 in 52 countries (Bloom, D.E, Canning, D., & Sevilla, J (2003) The Effect of Health on Economic Growth: A Production Function Approach. World Development 32(1): 1-13).
b) Investments in health are important safety nets against poverty traps in times of economic upheaval. Lack of health insurance in India means that over 37 million Indians fall below the poverty line each year due to catastrophic health spending; families will often sell assets like livestock in order to meet medical expenses.
c) Public financing of health services frees the poor to use more money to improve their welfare and create jobs for others. For example, in South Africa, 48% of health spending flowed via private intermediaries in the way of private health insurance contributions (40.7%) and the remainder is out of pocket spending. If the households did not have to spend this on health, they would either save it or spend it on other goods and services including investing in other household assets, and other activities that create jobs in the economy.
59. In Mexico the introduction of universal coverage linked to innovative initiatives to tackle their double burden of disease enhanced the basic capabilities of families living in extreme poverty. The interventions included basic sanitation, reproductive health, nutritional and growth surveillance, and specific prevention measures mostly for communicable diseases, but increasingly also for high blood pressure, diabetes and injury (Frenk 2006).
60. The country will have a healthier workforce at a lower cost in the long term, which increases employment and attracts foreign direct investment. For instance, Canada‟s provinces introduced national health insurance on a staggered basis from 1961 - 1975. Across 8 industries in 10 provinces, employment rose after the introduction of National Health insurance; wages increased as well, but average hours were unchanged. In addition, provinces with high initial levels of private insurance coverage had lower rates of employment and slower wage growth.
7.1 Economic Impact Modelling12
61. Macro-economic modelling undertaken suggests that the implementation of National Health Insurance could have positive or negative implications, depending on the model utilized and its outcomes. When implemented successfully, the National Health Insurance can improve employment and growth in the long-run. The economic impact assessment indicates that the National Health Insurance can have positive impacts in the long-run provided that it succeeds in improving the health indicators of the country, including significant improvement in life expectancy and child mortality. The better health outcomes need to translate into significant labour productivity. In the long-run, the higher productivity can lead to growth improving by 0.5 percentage points. However for National Health Insurance to have this positive macro-economic implication it needs to address the current institutional and staff constraints, improve significantly South Africa‟s health indicators, achieve the productivity gains and remain affordable.
8. THE THREE DIMENSIONS OF UNIVERSAL COVERAGE
62. In the 2010 World Health Report, the WHO provides guidance to countries on achieving universal healthcare coverage and social solidarity. It recommends three dimensions of progressing towards universal coverage and these have been identified as follows:
a) Population Coverage
It refers to the proportion of the population that has access to needed health services.
b) Service Coverage
It refers to the extent to which a range of services necessary to address health needs of the entire population are covered.
c) Financial Risk Protection
It refers to the extent to which the population is protected from catastrophic health expenditure particularly for households.
63. In a simplified diagrammatic form, the three dimensions may be summarized in the following figure:
Figure 1: The three dimensions of moving towards universal coverage
a) Length of the cube
This refers to the population coverage under universal coverage where the whole cube is covered and not just a portion of it.
b) Breadth of the cube
This refers to services covered. The present system wrongly confuses healthcare with treatment of diseases. A comprehensive healthcare package includes:
- Prevention of diseases,
- Promotion of health,
- Treatment of diseases where prevention has failed,
- Rehabilitative services
c) Height of the cube
This refers to the extent to which individual households are protected from exposure to financial risks associated with health. As previously stated, households exposed to financial risks due to illnesses are sometimes driven into poverty. 23
9. POPULATION COVERAGE UNDER NATIONAL HEALTH INSURANCE
64. National Health Insurance will cover all South Africans and legal permanent residents. Short-term residents, foreign students and tourists will be required to obtain compulsory travel insurance and must produce evidence of this upon entry into South Africa. Refugees and asylum seekers will be covered in line with provisions of the Refugees Act, 1998 and International Human Rights Instruments that have been ratified by the State.
65. In extending coverage the population that is in greatest need should be defined and the coverage must include those experiencing greatest difficulty in obtaining care. The identification of the population with the greatest need will be based on objective criteria.
10. THE RE-ENGINEERED PRIMARY HEALTH CARE SYSTEM
66. The strengthening of the South African health system will be based on a Primary Health Care approach. This will be rooted in the primary health care philosophy. The centrality of Primary Health Care was more clearly outlined by the WHO in the international conference on PHC held in Alma Ata, Kazakstan in 1978 when they redefined health as follows:
"Health is not just the absence of disease or infirmity but a state of complete physical, mental and social wellbeing. It is a fundamental human right and the attainment of the highest possible level of health is the most important worldwide social goal whose realisation requires action from many other social and economic sectors in addition to the health sector".
In South Africa, PHC services will be re-engineered to focus mainly community outreach services. Ongoing efforts to reengineer the PHC approach will ensure that the composition of a defined comprehensive primary care package of services extends beyond services traditionally provided in health facilities such as clinics, community health centres and district hospitals.
67. Primary health care services will be re-engineered to focus mainly on health promotion, preventative care, whilst also ensuring that quality curative and rehabilitative services appropriate to this level of care are rendered. Work is already underway in the National and Provincial Departments of Health to support the delivery of primary health care services. These services will be population orientated with extensive community outreach and home based services, and in which community health workers form an essential part. The district health system (DHS) will be the vehicle by which all PHC is delivered.
68. It has been shown that there is a strong support for inclusion of Primary Health Care services within the benefit package for mandatory insurance. This should also include private sector primary care services. This has the potential to reduce the disparities that exist in the distribution of human resources between the public and private sector.
69. All members of the population will be entitled to a defined comprehensive package of health services at all levels of care namely: primary, secondary, tertiary and quaternary with guaranteed continuity of healthcare benefits.
70. Primary health care services shall be delivered according to the following three streams:
a) District-based clinical specialist support teams supporting delivery of priority health care programmes at a district
b) School-based Primary Health Care services
c) Municipal Ward-based Primary Health Care Agents
10.1 District Clinical Specialist Support Teams
71. In order to address high levels of maternal and child mortality and to improve health outcomes, an integrated team of specialists will be based in the districts. The specialities will include: a principal obstetrician and gynaecologist; a principal paediatrician; a principal family physician; a principal anaesthetist; a principal midwife and a principal primary health care professional nurse. Others will be added over time as the need arises. The role of these teams will be to provide clinical support and oversight particularly in those districts with a high disease burden.
72. The health districts in South Africa have for a long time lacked specialist resources to provide support to primary healthcare services. With the increased shortage in specialist health professionals, the gap in specialist support has become wider and continues to reduce access for vulnerable populations and increases the total cost of medical care. The objectives of the district clinical specialist support teams will be :
- To promote innovative models of providing specialist healthcare closer to the patients‟ home
- To promote integrated working practices between GPs and hospital based specialists
- To improve the quality of services rendered at the first level of care by ensuring adherence to treatment guidelines and protocols
- To provide peer support for specialists working in primary care.
73. These innovative approaches can improve access, outcomes and service utilisation especially when delivered as a multi-faceted approach. Evidence from the Cochrane systematic review indicates that in contexts where specialist medical practitioners have been involved in primary care clinics and rural hospital settings it has led to increasing the accessibility and effectiveness of specialist services and their integration with primary care services (Gruen, et al. 2009). Contrary to the norm of clinical specialist outreach services, these are not outreach specialists. They will be an integral and permanent feature of health care delivery in South Africa. The medical schools in the country should be able to provide these teams, even if it is on a rotational basis.
This model is also cost effective as patients will be seen early by specialists before they are too ill and need advanced technology and treatment at higher levels. It will also address the problems associated with delays in referral or poor access to needed specialist services.
10.2 School Health Services
74. School health services will be delivered by a team that is headed by a professional nurse. The services will include health promotion, prevention and curative health services that address the health needs of school-going children, including those children who have missed the opportunity to access services such as child immunization services during their pre-school years.
75. School health is an integral part of the comprehensive package of primary health care services that must be delivered to every school in the district. The school-based health programme will ensure that the general state of physical, mental health and well-being of school going children including pre-Grade R, and Grade R up until Grade 12.
76. The other areas of the school health programme will include a focus on child and sex abuse, oral health services, vision screening services, eradication of parasites, nutritional services, substance abuse, sexual and reproductive health rights including family planning services, and HIV and AIDS related programmes.
10.3 Municipal Ward-based Primary Health Care Agents
77. A team of PHC agents will be deployed in every municipal ward. At least 10 people will be deployed per ward. Each team will be headed by a health professional depending on availability. Each member of the team will be allocated a certain number of families.
78. The teams will collectively facilitate community involvement and participation in identifying health problems and behaviours that place individuals at risk of disease or injury; vulnerable individuals and groups; and implementing appropriate interventions from the service package to address the behaviours or health problems.
11. HEALTHCARE BENEFITS UNDER NATIONAL HEALTH INSURANCE
79. The provision of a comprehensive benefit package of care under National Health Insurance will be fair and rational. The term „benefit package‟ describes how different types of services are organized into different levels of care in the public sector (J Doherty, 2010). It also defines the types of services that are considered as achievable for the country commensurate with its resources.
80. The National Department of Health (NDOH) has over the number of years developed „benefit packages,‟ for primary health care, district hospital services, regional hospital services and tertiary services. Despite this, barriers to accessing these packages still exist.
81. In the design of these packages, certain considerations should be made to overcome the identified barriers to access. A review of the international evidence on high-level strategies to promote health and health equity found that comprehensive benefit packages should be determined first by considering which interventions are important in improving access, offering financial protection to less advantaged groups and enhancing redistribution of healthcare services. The comprehensiveness of the package of services to be provided must also demonstrate how well the health system is performing, and ensure timely referral of patients at different levels of care.
82. The norms and standards for the package to be provided in the district will assist in outlining precisely the measurable targets which must be achieved and the acceptable standards of care which providers must comply with. These will enable managers at facility, district, provincial and national levels to compare performance and challenges between individual and groups of similar facilities.
11.1 The Service Package within the Context of District Heath Services
83. Services provided within the context of the district health system have shown mixed results purely because they have been viewed as a once off process of granting authority to lower levels of administration in a decentralised manner. Evidence shows that this must be a carefully planned process that requires good administrative systems with innovative service delivery approaches that would bring about efficiency, improved management including financial management.
84. A district health package of public health and clinical interventions, which are highly cost-effective and deal with major sources of disease burden, through the three PHC streams involving various teams, can be provided in South Africa at reasonable cost. Properly delivered through the primary health care streams, this package could eliminate 21% to 38% of the burden of premature mortality and disability in children under 15-years of age, and 10% to 18% of the burden in adults (Bobadilla, 1994).The district health package is designed to meet the needs of the population. Some of the issues to be addressed are:
- Availability of health services at adequately convenient hours with enough professional staff to attend to their needs
- Consideration of the user's privacy, confidentiality, fair treatment by staff members and ensuring the user's dignity is respected at all times
- Compliance with core quality standards
11.2 Delivery of Primary Health Care Services through Private Providers
85. In addition to the three streams, PHC services will be delivered through accredited and contracted private providers practicing within a District. A sizeable proportion of the population in the country uses private providers for their health care needs and more often than not it involves substantial out of pocket payment.
86. There are several ways in which private providers could participate in providing PHC services to the population. The salient feature of contracting private providers in the delivery of primary health care services will entail the specification of the range of services that will be provided. These may include services by the general practitioners to patients who must get the full range of primary care services required in one facility or comparable arrangement which does not inconvenience or require travel costs on the part of the patient.
11.3 Hospital-Based Benefits
87. Services to be rendered at the hospital level will be based on a defined comprehensive package that is appropriate to the level of care and referral systems13. The National Health Insurance will provide an evidenced-based comprehensive package of health services which includes all levels of care namely: primary, secondary, tertiary and quaternary health care services.
11.4 Designation of Hospitals
88. As part of the overhaul of the health system and improvement of its management, hospitals in South Africa will be re-designated as follows:
- District hospital;
- Regional hospital;
- Tertiary hospital;
- Central hospital; and
- Specialized hospital.
Each level of hospital designation will be managed at a newly defined level with appropriate qualifications and skills as defined by the National Health Council.
89. It is recognized that health care services in South Africa are rendered at different levels of care with specific core packages. Patients and/or members of the public should be able to access the care needed at the time of need. This should be part of the system design and operations with appropriate guarantee of patient safety.
District hospitals
90. This is the smallest type of hospital which provides generalist medical services. In terms of specialist care, they are limited to four basic areas namely:
- Obstetrics and Gynaecology
- Paediatrics and Child Health
- General Surgery
- Family Medicine
91. The package of care provided at district hospitals includes trauma and emergency care, in-patient care, out-patient visits, rehabilitation services, geriatric care, laboratory and diagnostic services, paediatric and obstetric care.
92. Consequently in the South African context these facilities will have anaesthesia administered at the general practitioner level, within a theatre complex. These facilities will be supported by the district specialist teams within a broad PHC service package.
Regional Hospitals
93. The regional hospitals will offer a range of general specialist services. Hospitals at this level render services at a general specialist level, receive referrals from district hospitals and provide specialist services to a number of district hospitals (preferably six or less). The eight general specialist services that will be provided is general surgery, orthopaedics, general medicine, paediatrics, obstetrics & gynaecology, psychiatry, radiology and anaesthetics.
Tertiary Hospitals
94. Tertiary hospitals render super specialist and sub specialist care. They also serve as a main platform for training of health workers and research. Most care provided in these hospitals, requires the expertise of teams led by experienced specialists. This includes cardiology, cardiothoracic surgery, craniofacial surgery, diagnostic radiology, ear, nose and throat (ENT), endocrinology, geriatrics, haematology, human genetics, infectious diseases, general surgery, orthopaedics, general medicine, paediatrics, obstetrics & gynaecology, radiology and anaesthetics. These services may be included in more developed tertiary services Cardiothoracic Surgery, Renal Transplant, Neurosurgery, Oncology, Nuclear Medicine, and a range of Paediatric sub-specialties.
Central Hospitals
95. These are national referral hospitals that are attached to a medical school and provide a training platform for the training of health professionals and research. Central hospitals render very highly specialized tertiary and quaternary service on a national basis. It also functions as highly specialized referral units for the other hospitals. These hospitals employ high technology and highly trained staff.
Specialized hospitals
96. The specialized hospitals are usually one disciple focused and are extremely vertical in the range of services offered at the hospital. There are a wide range of possible specialties that could be focused in a hospital, the two most common being TB and Psychiatry, but they may also include spinal injuries, maternity, heart, orthopaedics, urology and infectious diseases. These units may also provide either acute, sub acute or chronic care or all of four levels of care.
12. ACCREDITATION OF PROVIDERS OF HEALTH CARE SERVICES
12.1The Office of Health Standards Compliance
97. The Office of Health Standards Compliance (OHSC) will be established through an Act of Parliament. It will have three units, namely: inspection, norms and standards and the office of the ombudsperson. It will set norms and standards and undertake the inspection of all health facilities. This process will be undertaken in close collaboration with the implementation of quality improvement plans to ensure facilities are ready for accreditation and contracting with the National Health Insurance. Interim assessments, focusing on high-risk elements in public health facilities, will be conducted within regular intervals to ensure that set standards are maintained. Recommendations will be made on the introduction of continuous quality improvement in public healthcare facilities, with associated training.
98. The OHSC will facilitate the development of multidisciplinary organisational standards for healthcare facilities using evidence-based principles for standard development to evaluate compliance and to monitor progress. The certification process will enable management at all levels of the health system to use the information generated to make informed decisions about quality improvement.
99. All health establishments (public and private) that wish to be considered for rendering health services to the population will have to meet set standards of quality. There are six core standards that form part of a comprehensive quality package. These standards deal with key quality principles that will improve safety and facilitate access to healthcare services. These standards will form only one aspect of accreditation, other criteria for accreditation will include service elements, management systems, performance standards and coverage.
12.2 Accreditation Standards
100. The accreditation standards will specify the minimum range of services to be provided at different levels of care. Central to the accreditation is the provision of primary health care services that can demonstrate performance linked to health outcomes. This will entail involvement of competent health and medical staff with appropriate skills. In addition, providers at all levels of care must adhere to the referral procedures as defined by the National Health Insurance and the referral system will be clearly defined for services within and outside the health sub-district, district and province to assure continuity of care and effective cost containment.
13. PAYMENT OF PROVIDERS UNDER NATIONAL HEALTH INSURANCE
101. In order to ensure effective cost-containment and the future sustainability of the National Health Insurance, existing provider payment mechanisms and associated accountability processes will be changed.
102. At the primary care level, accredited providers will be reimbursed using a risk-adjusted capitation system linked to a performance-based mechanism. The annual capitation amount will be linked to the size of the registered population, epidemiological profile, target utilization and cost levels.
103. At the hospital level, accredited and contracted facilities will be reimbursed using global budgets in the initial phases of implementation with a gradual migration towards diagnosis related groups (DRGs) with a strong emphasis on performance management.
104. In preparation for contracting with private providers, mechanisms for achieving cost-efficiency will be investigated including international benchmarking from countries of similar economic development that have successfully implemented such processes.
105. Public emergency medical services will be reimbursed through the public hospital global budget initially and a case-based mechanism as the system matures. Contracted private emergency services will be reimbursed using a case-based approach.
106. The provider payment mechanisms must ensure incentives for the health workers and professionals in the public sector and it is also important to consider the implementation of performance-based payment mechanisms.
107. While capitation should be maintained as one of the basic forms of provider reimbursement, adjustment should be made in its application, with the following principles:
a) the capitation amount will be a uniform amount for the defined levels of providers;
b) the capitation amount should be linked to an appropriate index;
c) the public and private health providers contracted by the National Health Insurance, will be assisted in controlling the expenditure through recommended formula, and adherence to treatment protocols for all conditions covered under the defined package of care. This will be necessary to ensure the appropriate level of service provision and avoid under-servicing which is a common characteristic of many capitation-based systems; and
d) the budgets will be calculated on the basis of a risk-adjusted capitation formula taking into account key factors such as population size, age and gender and disease/epidemiological profile.
13.1 HEALTHCARE CODING SYSTEMS AND REIMBURSEMENT
108. Coding systems are an important component of health informatics and reimbursement. National Health Insurance will adopt a coding system that allows providers to uniformly report on the services rendered or goods provided for the purpose of reimbursement. The coding system must allocate a code relating to a particular service so that the National Health Insurance would be able to reimburse for the service with a full understanding of the service delivered or goods supplied. It is also important that the coding system provides the necessary health information on the burden of disease for the purposes of planning and decision making.
109. The reimbursement system for inpatient services will be according to disease related groups. A case mix or grouper system will be adapted for the South African environment drawing on good practices that are internationally accepted and have been successfully implemented in other jurisdictions.
13.2 UNIT OF CONTRACTING PROVIDERS OF HEALTH CARE SERVICES
110. It is envisaged that the District Health Authority, as part of the health service provision system, will be established and given the responsibility of contracting with the National Health Insurance in the purchasing decisions for health services. The District Health Authority as a contracting unit will be supported by the National Health Insurance Fund‟s sub-national offices to manage the various contracts with accredited providers.
111. A further role of the District Health Authority will be to ensure that services that are planned for are adequate and accessible for the population that is located within a defined health district. Initially all districts may not be able to participate in purchasing decisions due to capacity constraints. Nonetheless, over a period of time, District Management teams will be strengthened.
112. Accredited providers will be contracted and reimbursed on the basis of the payment levels determined by the National Health Insurance. Accreditation will also take into account the need for particular providers within a particular area, type of health services required as well as available resources within the district. The District Health Authority will monitor the performance of contracted providers within a district and performance will be linked to a reimbursement mechanism that is aimed at improving health outcomes in the district.
113. There will be a separation of the functions of purchasing and provision of services within the National Health Insurance. A clear delineation of the roles and functions of provincial and national spheres of government on the one hand and National Health Insurance will be undertaken in order to ensure an effective purchaser - provider split. The purpose of this is to avoid the potential duplication of administrative processes so as to minimise administration costs.
14. PRINCIPAL FUNDING MECHANISMS FOR NATIONAL HEALTH INSURANCE
114. Universal coverage to affordable health care services is best achieved through a prepayment health financing mechanism. To achieve universal coverage, pooling of funds requires that payments for health care are made in advance of an illness, and these payments are pooled and used to fund health services for the population. The funds can be from a combination of sources (e.g. the fiscus, employers and individuals). The precise combination of these sources is the subject of continuing technical work and will be further clarified in the next 6 months in parallel to the public consultation.
115. An important consideration is that the revenue base should be as broad as possible in order to achieve the lowest contribution rates and still generate sufficient funds to supplement the general tax allocation to the National Health Insurance. As the National Health Insurance matures, consideration will be given to the alignment and consolidation of health benefits offered by other relevant statutory entities.
14.1 The Role of Co-Payments under National Health Insurance
116. Ordinarily universal coverage does not encourage co-payments. Even the WHO does not encourage co-payments, and National Health Insurance will not be an exception. However, there are instances under which National Health Insurance may be forced to impose co-payments, and these may include amongst others:
a) Services rendered not in accordance with the National Health Insurance treatment protocols and guidelines;
b) Health care benefits that are not covered under the National Health Insurance benefit package (e.g. originator drugs or expensive spectacle frames)
c) Non-adherence to the appropriately defined referral system
d) Services that are rendered by providers that are not accredited and contracted by National Health Insurance
e) Health services utilised by non-insured persons (such as tourists)
15. HOW MUCH WILL NATIONAL HEALTH INSURANCE COST
117. The costing estimates presented in this section focus on providing an indication of the estimated resource requirements for achieving universal coverage, based on cost effective delivery of health services.
118. It is not possible to model with 100% accuracy the precise resource requirements of the future National Health Insurance, but the figures presented provide a good indication of the likely magnitude of resource requirements and more importantly allow for the implications of key National Health Insurance design elements (e.g. of different benefit packages) to be assessed. The figures presented here are preliminary estimates of the resource requirements for the National Health Insurance. The costing of the National Health Insurance is an iterative process and further work will be undertaken to refine cost estimates to take account of detailed proposals being developed, particularly in relation to strategies for gate-keeping at primary care level and provider payment mechanisms to avoid over-utilisation and over-provision of services.
119. The costing model used in this preliminary costing adopts the approach recommended by the International Labour Office (ILO), which is:
Total expenditure = user population X service utilisation rates X unit costs
It takes account of the population size and how population will grow over time as well as the age and sex composition of the current and future population (as young children, the elderly and women of childbearing age have greater health service needs). It also takes into account how frequently different groups use different health services and how this may change over time, particularly when financial barriers to access are removed under the National Health Insurance. Finally, it considers how much it costs (now and in future) to provide each type of health service drawing on the current costs of provision of public sector services and the need to dramatically improve resourcing of public sector health services.
120. The model presents the estimated resource requirements using a „public sector framework‟. This implies that a defined comprehensive package of services is provided for all South Africans, but this package is not specified as in current medical schemes in terms of specific services that will be covered (e.g. whether or not chronic medicines for depression are covered). Instead, the comprehensive package is defined in terms of individuals having access to primary care facilities and to specialist and hospital care on referral. For each of these broad categories of services, there are „norms‟ in relation to the type of staff that should be employed, equipment that should be available and the range of services that should be provided. In addition, it is based on public sector unit costs, but at substantially improved resourcing levels than at present.
121. The improvement in resourcing is phased in over the initial 7 year period (i.e. it is regarded as an urgent intervention). The model makes allowance for large increases in utilisation when financial barriers to service use are removed under the National Health Insurance (of over 70% in outpatient care and about 80% in inpatient care for those who are currently „uninsured‟ relative to their current utilisation levels). These projected increases in utilisation are comparable to the extent of utilisation increases experienced in Thailand when a universal health coverage system was introduced. It will take considerable time for the supply capacity (facilities and health professionals) to grow to accommodate such utilisation increases. For this reason, these increases are phased in over a 14 year period.
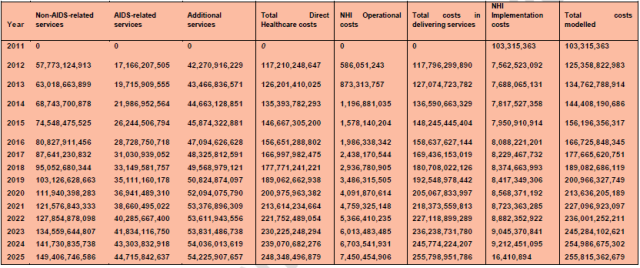
122. This model indicates that resource requirements under this model increases from R125 billion in 2012 to R214 billion in 2020 and R255 billion in 2025 if implemented gradually over a 14-year period. These figures are expressed in real terms (i.e. these are the values in real 2010 financial terms).
123. These figures should be placed within the context of current spending levels. The 2010/11 health MTEF budget is R101 billion and increases to R110 billion in 2012/13 (2010 prices). This does not include spending by other departments (such as health spending by Defence and Correctional Services). In addition, a similar amount is being spent on medical scheme contributions (totalling R90 billion (2010 prices)) in 2009 - the most recent year for which audited figures are availablei - and estimated to total about R92 billion in 2010 based on the rate of increase between 2006 and 2008). This represents a total of over R227 billion being spent on health services in South Africa in 2010, which is equivalent to almost 8.5% of GDP.
124. Table 1 below shows preliminary cost estimates of the health care package, implementation as well as administration costs. Further costing will be undertaken by the National Treasury and the Department of Health to further refine the model and to look at long term fiscal implications and effects of the National Health Insurance contribution on households.
Table 1: Healthcare delivery and National Health Insurance implementation Preliminary Cost estimates 2011 - 2025
|
Year |
Non-AIDS-related services |
AIDS-related services |
Additional services |
Total Direct Healthcare costs |
NHI Operational costs |
NHI Implementation costs |
|
% of total in 2012 |
46.10% |
13.70% |
33.70% |
93.50% |
0.50% |
6.00% |
|
% of total in 2025 |
58.40% |
17.50% |
21.20% |
97.10% |
2.90% |
0.00% |
125. It should be noted that increased spending on the National Health Insurance will be partially offset by the likely decline in spending on medical schemes (as all South Africans will be entitled to benefit from National Health Insurance services). In addition, National Treasury is projecting real GDP growth of 3.1% in 2010/11, 3.6% in 2011/12 and 4.2% in 2012/13. National Health Insurance will require an increase in spending on health care from public resources (general tax revenue and a mandatory National Health Insurance contribution) that is faster than projected GDP increases. However, the ultimate level of spending on a universal health system relative to GDP (of 6.2%) is less than current spending by government and via medical schemes (of 8.5%).
126. This National Health Insurance contribution should be compared to the current level of medical scheme contributions. Based on data from the 2005/06 Income and Expenditure Survey, the overall average level of contributions for all medical scheme members is over 9% of income. The lowest income medical scheme members currently contribute over 14% of their income to medical schemes (for the lowest 40% of scheme members), the middle 20% of scheme members spend nearly 12% of income on medical scheme contributions, the second wealthiest 20% of medical scheme members devote over 9% of their income to contributions while the richest 20% of scheme members devote about 5.5% of their income to medical scheme contributions. The intention is that the National Health Insurance benefits, to which all South Africans will be entitled, will be of sufficient range and quality that South Africans have a real choice as to whether to continue medical scheme membership or simply draw on their National Health Insurance entitlements.
127. The preliminary costing estimates provided above indicate that the National Health Insurance is affordable for South Africa. However, the present system of fragmentation, associated with the high cost, curative and hospi-centric approach and excessive and unjustifiable charges, especially within the private health sector is unsustainable. No amount of funding will be sufficient to ensure the sustainability of National Health Insurance unless the systemic challenges within the health system are also addressed.
128. The challenges of sustainable financing do not apply only to South Africa but have also been experienced in other countries that follow the route that is currently dominant in the South African private health sector. An example of this problem has been experienced in the United States of America (USA) where the concentrated private hospital and specialists' market power coupled with a fee-for-service reimbursement system that promotes over-servicing of patients has resulted in a high cost, curative care.
129. The high cost, curative and hospi-centric system cannot be sustainable not only for the implementation of National Health Insurance but also for any form of healthcare financing mechanism including the present medical schemes environment. In order to effectively implement such a large health systems reform programme, strengthening of the public health system and transformation of the health services delivery platform is critical for the success of National Health Insurance.
15.1 Funding Flows
130. All revenue collection would be undertaken by the South African Revenue Services (SARS), including the mandatory contribution. All funding for personal health care services will flow through the National Health Insurance Fund. Treasury will allocate general tax revenue for personal healthcare services and the payroll-linked mandatory contribution to National Health Insurance in consultation with the Minister of Health and the National Health Insurance.
16. THE ESTABLISHMENT OF THE NATIONAL HEALTH INSURANCE FUND
131. In order to implement an effective National Health Insurance, there will be a reconfiguration of the institutions and organisations involved in the funding, pooling, purchasing and provision of health care services in the South African health system.
132. The National Health Insurance Fund will be established as a government-owned entity that is publicly administered. It will be a single payer entity with sub-national offices to manage nationally negotiated contracts with all appropriately accredited and contracted healthcare providers. The covered services will be defined as a comprehensive package of services that includes personal care, health prevention and promotion services. The main responsibility of the National Health Insurance Fund will be to pool funds and use these funds to purchase health services on behalf of the entire population from contracted public and private health care providers. Nonetheless, a multi-payer system in a National Health Insurance will also be explored as an alternative to the preferred single-funder, single-purchaser publicly administered Fund.
133. The National Health Insurance Fund will be an autonomous public entity reporting to the Minister of Health and Parliament. It will be governed by the relevant statutes. The Fund will be established through the passing of enabling legislation and supporting regulations. The Minister of Health will have oversight of the National Health Insurance Fund.
134. The Department of Health will continue to play its overall stewardship role of the health system, such as development of overall health policy, planning to meet changes in the country's health care needs as determined by changes in population demography, epidemiological profile, health technology and any other relevant developments. The Department of Health will also remain a major provider of services through its national, provincial and district level structures and facilities. Furthermore, the Department of Health will continue to provide non-personal services including overall responsibility for infrastructure development and direction of health worker training and planning. The responsibility of coordinating the development of overall health plans including personal services will be retained within the Department of Health. The National Health Insurance Fund will purchase personal services in accordance with the approved plans by the National and Provincial Departments of Health.
135. At the national level, the National Health Insurance Fund will be managed by a Chief Executive Officer (CEO) who will report directly to the Minister of Health. The CEO will be supported by a competent Executive Management Team and specific technical committees including the technical advisory committee, audit committee, pricing committee, remuneration committee, benefits advisory committee and others.
136. The National Health Insurance Fund will be advised by a technical advisory committee made up of experts in health care financing, health economics, medical and nursing services, pharmaceutical services, public health planning, research, monitoring and evaluation, public health law, labour, administration of public insurance schemes, actuarial sciences, information technology and communication. At a sub-national level, the National Health Insurance Fund will establish sub-national structures that will be responsible for managing the nationally negotiated contracts with the District Health Authorities that are located within particular health districts.
17. THE ROLE OF MEDICAL SCHEMES
137. Membership to the National Health Insurance will be mandatory for all South Africans. Nevertheless, it will be up to the general public to continue with voluntary private medical scheme membership if they choose to. Accordingly, medical schemes will continue to exist alongside National Health Insurance. However, there will be no tax subsidies for those who choose to continue with medical scheme cover.
138. The exact form of services that medical schemes will offer may evolve to include top-up insurance. However, no South African and legal permanent resident can opt out of contributing to National Health Insurance even if they retain their medical scheme membership.
139. There is existing expertise residing in the health sector in the area of administration and management of insurance funds. Where necessary and relevant, this expertise may be drawn upon within the single payer publicly administered National Health Insurance, to ensure that adequate in-house capacity is developed.
18. REGISTRATION OF THE POPULATION
140. The National Health Insurance Fund will only deal with registered citizens as provided by the Department of Home Affairs. Only those registered will have access to the defined comprehensive package of services. Accredited and contracted health providers will provide services to the registered population.
141. A National Health Insurance card will be issued for the registered population and it will allow for ease of access to patient information and for the portability of health services. The National Health Insurance card will be the same for the entire population, regardless of their contributory or other status, in order to avoid the stigma that may be associated with subsidised households and individuals.
19. INFORMATION SYSTEMS FOR NATIONAL HEALTH INSURANCE
142. The National Health Insurance will contribute to an integrated and enhanced National Health Information System. National Health Insurance information system will contribute towards the determination of the population‟s health needs and outcomes. The information system will also be essential for portability of services for the population. The National Health Insurance information system will be based on an electronic platform, with linkages between the National Health Insurance membership data base (with updated contribution status) and accredited and contracted health care providers. The information system will need to be adequately budgeted for in the initial stage to help ensure effective implementation. Developmental work will be conducted on a National Health Insurance patient card and supporting information platform.
20. MIGRATION FROM THE CURRENT HEALTH SYSTEM INTO THE NATIONAL HEALTH INSURANCE ENVIRONMENT
143. The transitional process from the current to the proposed National Health Insurance environment within the South African health system will require a well-articulated implementation plan. The implementation of National Health Insurance will be done in a phased and systematic manner at both the national and sub-national levels. The migration period will occur in three phases over the fourteen years of implementation.
144. The initial phases of implementation will include the real-life demonstration of the key administrative and technical aspects of National Health Insurance so as to ensure the smooth roll-out of the systems as it matures and new information becomes available. A number of interrelated elements must be carefully addressed to ensure an effective transition process. These elements include:
145. Development of a strategy that allows for the strengthening of district health structures to support service delivery within the National Health Insurance. This will entail accelerating the re-engineering of the Primary Health Care Approach through the incremental establishment of Municipal Ward-based family health teams, District-based specialist teams and the roll-out of the school-based health programmes. The strengthening of the District Health Management teams will be accelerated to improve the capacity to contract with the National Health Insurance Fund by the District Health Authority;
146. Development and implementation of a comprehensive plan for quality improvement, assurance and compliance for all providers supported by the Office of Health Standards Compliance. The Office of Health Standards Compliance will inspect, licence and certify all health care facilities. The National Health Insurance Fund will contract with accredited health care providers based on prescribed criteria and standards;
147. Determination of a transition and long term plan for addressing the current Human Resources (HR) shortages in the health system. This will include increasing capacity of nursing colleges and health science faculties to produce more health professionals. Furthermore, mobilisation of additional financial and HR resources will be undertaken to support enhanced health systems delivery within the National Health Insurance;
148. Conducting real-life demonstrations and pilots in prioritized health districts on the management capacity, appropriateness of the service package, and ability of the accredited and contracted providers to deliver on the defined comprehensive package of health services to be provided at the appropriate level of care. The prioritized districts will be selected based on demographic, socio-economic and epidemiological profiles as well as management functionality at the selected health districts;
149. The assessment of existing health infrastructure (including facilities, technology and management capacity) in the country and a plan to improve its capacity and effectiveness to support health services delivery and provision within the National Health Insurance;
150. Implementation of hospitals management reforms that include governance reforms, improvements in financial management, decentralization of authority associated with hospital management autonomy and accountability;
151. Development of a plan that informs the processes around implementing innovative purchasing and procurement processes to allow the National Health Insurance to yield the best economies of scale;
152. Development of an integrated plan to support processes around population registration. This plan must be informed by building on existing capacities in the country and through involving various stakeholders. The plan will also include conducting research on the type of National Health Insurance Card that will be used to allow the ensured population to be identified, access the defined comprehensive cover and benefit from the portability of health care benefits;
153. Further refinement of the financial resource envelope that will be required to adequately fund the National Health Insurance and service delivery platforms at the primary secondary, tertiary and quaternary levels, including the concurrent health systems strengthening activities that are informed by the Department of Health's Ten Point Plan;
154. Refinement of the revenue mobilisation strategy and pooling systems that will be implemented to ensure National Health Insurance provides the appropriate financial risk protection for the entire population and yields the full economies of scale from the publicly administered monopsony structure to support the single-purchaser National Health Insurance. This will also include alignment of health benefits and tariff system under the Road Accident Fund, Compensation for Occupational Diseases and Injuries, Compensation Commission for Occupational Diseases and the Occupational Diseases in Mines and Works Act.
155. Refinement of the provider payment mechanisms strategies and implementation of interim mechanisms to move from the current reimbursement system to the proposed performance-based payment system under the National Health Insurance;
156. Development of a detailed transition process from the current fragmented health information system to an integrated health information system that supports efficiency, effectiveness, information portability, confidentiality and enhanced proactive decision making and system planning.
157. Review of existing legislative and regulatory laws to inform the preparation of the Bill/Act that will create an enabling environment for the implementation of the National Health Insurance in South Africa. Furthermore, passing of an enabling legislation to establish the National Health Insurance Fund will be undertaken. The fund will be established initially as a national office and later to sub-national offices at provinces.
158. A National Health Insurance Conditional Grant will be allocated to the National Department of Health as part of the resource allocation processes intended to support activities directed at piloting key aspect of the National Health Insurance. These resources will be used to fund the shadow processes for implementing and rolling out of the key service delivery, administrative and technical functions required by the National Health Insurance in the initial years.
159. A summary of some of the key elements that will be addressed through the phased implementation are shown in following tables:
Table 1: Phasing-In of National Health Insurance - The First 5 years
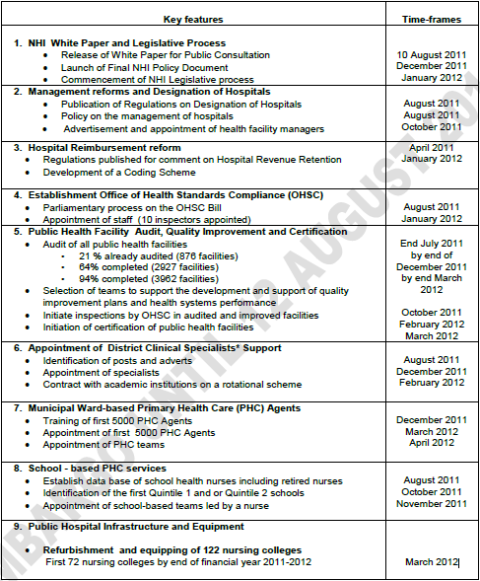
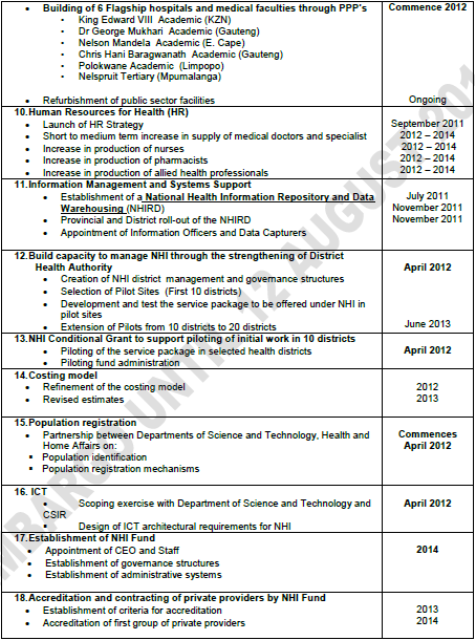
Table 3: Phasing-In of National Health Insurance - Second Phase (2016-2020)
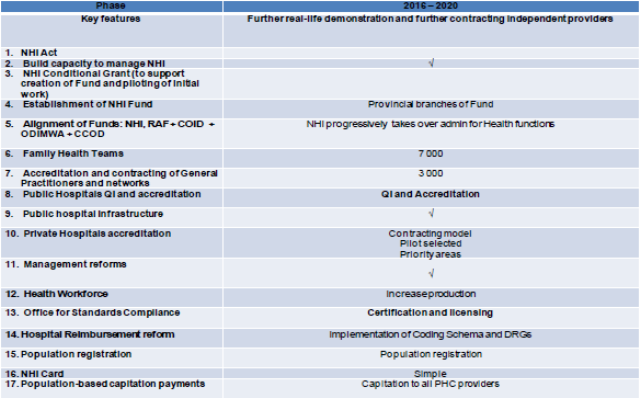
Table 3: Phasing-In of National Health Insurance - Third Phase (2021-2025)
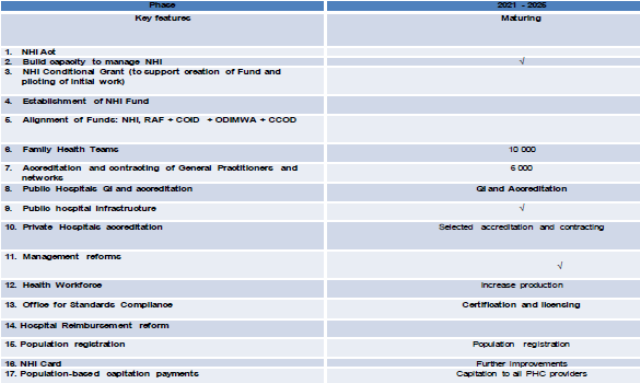
BIBILOGRAPHY
WHO.The World Health Report (2008): Primary Health Care - Now More than Ever.
Sara Bennett and Lucy Gilson (2001) Pro-poor policies - Health financing: designing and implementing; HSRC- DFID Health Systems Resource Centre
Coovadia, H., Jewkes, R., Barron, P. Sanders, D., McIntyre, D. (2009): The Health and Health System of South Africa: Historical Roots of Current Public Health Challenges. The Lancet 2009; 374: 817-34
George Schieber, Cristian Baeza, Daniel Kress, and Margaret Maier, "Financing Health Systems in the 21st Century." 2006. Disease Control Priorities in Developing Countries (2nd Edition), ed., 225-242. New York: Oxford University Press. DOI: 10.1596/978-0-821-36179-5/Chpt-12.
Bloom, D.E, Canning, D., & Sevilla, J (2003) The Effect of Health on Economic Growth: A Production Function Approach. World Development 32(1): 1-13.
Gruen, R.L, Weeramanthri, T., Knight S.S.E and Bailie R.S (2009) Specialist outreach clinics in primary care and rural hospital settings. Cochrane Database of Systematic Reviews 2003
Doherty, J. (2010) Specification of the Benefit Package Under NHI, September 2010.
Monograph commissioned by the Ministerial Advisory Committee on NHI.
McIntyre D (2010) National Health Insurance: Providing A Vocabulary for Public Engagement. In South African Health Review (2010) Padarath, A and Fonn, S eds. Health System Trust, Pretoria.
Bobadilla, J-L, C. (1994): Design, Content and Financing over an Essential National Package of Health Services. Geneva: WHO
National Treasury (2010). Budget Review. Pretoria: National Treasury.
Council for Medical Schemes (2009) Annual Report, 2008-09. Pretoria: Council for Medical Schemes.
Yu SH, Anderson GF. Achieving universal health insurance in Korea: a model for other developing countries? Health Policy. 1992; 20(3):289-99.
Soeters R, Griffiths F. Improving government health services through contract management: a case from Cambodia. Health Policy Plan. 2003 Mar; 18(1):74-83
Jack W. Contracting for health services: an evaluation of recent reforms in Nicaragua. Health Policy Plan. 2003 Jun; 18(2):195-204.
Contracting for Health Services: Lessons from New Zealand. World Health Organization 2004 URL: http://whqlibdoc.who.int/wpro/2004/9290610670.pdf
Bossert T et al. Decentralization in Zambia: resource allocation and district performance. Health Policy Plan. (2003)
Bossert TJ, Beauvais JC. Decentralization of health systems in Ghana, Zambia, Uganda and the Philippines: a comparative analysis of decision space. Health Policy Plan. 2002 Mar; 17(1):14-31.
Teerawattananon Y, Tangcharoensathien V. Designing a reproductive health services package in the universal health insurance scheme in Thailand: match and mismatch of need, demand and supply. Health Policy Plan. 2004 Oct; 19 Suppl 1:i31-i39.
Liu X, et al. The effectiveness of contracting-out primary health care services in developing countries: a review of the evidence. Health Policy Plan. 2008 Jan; 23(1):1-13.
Meng Q et al. Expanding health insurance coverage in vulnerable groups: a systematic review of options. Health Policy Plan. 2011 Mar; 26(2):93-104.
Julio Frenk. Bridging the divide: global lessons from evidence-based health policy in Mexico. Lancet 2006; 368: 954-61
Kwon S. Thirty years of national health insurance in South Korea: lessons for achieving universal health care coverage. Health Policy Plan. 2009 Jan; 24(1):63-71.
Agyepong IA, Adjei S. Public social policy development and implementation: a case study of the Ghana National Health Insurance scheme. Health Policy Plan. 2008 Mar; 23(2):150-60
Abramson WB. Monitoring and evaluation of contracts for health service delivery in Costa Rica. Health Policy Plan. 2001 Dec; 16(4):404-11.
Gilson L et al. The SAZA study: implementing health financing reform in South Africa and Zambia. Health Policy Plan. 2003 Mar; 18(1):31-46
Doherty J. Cost-effectiveness analysis for priority-setting in South Africa-what are the possibilities? S Afr Med J. 2010 Dec 1; 100(12):816-21.
McIntyre D. (2008) what progress in health care financing? Health Policy Plan. 2010 Sep; 25(5):349-51
Masiye F, et al. From targeted exemptions to user fee abolition in health care: experience from rural Zambia. Soc Sci Med. 2010 Aug; 71(4):743-50.
Carrin G, James C. Key performance indicators for the implementation of social health insurance. Appl Health Econ Health Policy. 2005; 4(1):15-22.
Devadasan N, Van Damme W. Payments for health care in India. Lancet. 2006 Dec 23; 368(9554):2209
De Allegri M et al. Understanding enrolment in community health insurance in sub-Saharan Africa: a population-based case-control study in rural Burkina Faso. Bull World Health Organ. 2006 Nov; 84(11):852-8.
Gilson L, et al. The equity impacts of community financing activities in three African countries. Int J Health Plann Manage. 2000 Oct-Dec; 15(4):291-317.
World Development Report 1993. Investing in Health. URL: http://files.dcp2.org/pdf/WorldDevelopmentReport1993.pdf
Mills A, et al (2000) The response of providers to capitation payment: a case-study from Thailand. Health Policy. Apr; 51(3):163-80
GLOSSARY OF KEY TERMS
Accreditation of Health Services Providers - The process through which an entity undertakes to certify healthcare and health services providers according to appropriate and specific criteria in order for them to be contracted and reimbursed for rendering services to a defined population.
Case Mix Reimbursement - This is a provider payment mechanism that uses case-based payment systems such as diagnostic-related groups (DRGs).The approach used is to bundle different pathologies or interventions into homogenous cost groups that are then ascribed an average treatment cost. It is commonly applied in the reimbursement of hospitals as an intervention to control costs and encourage efficiency in many countries, not just high-income settings.
Contracting of Health Services Providers - The process through which an entity enters into formal and legally binding arrangements with appropriately licensed and accredited healthcare and health services providers for rendering services to a defined population. The contractual arrangements may stipulate the rates for reimbursement of providers, the penalties and sanctions that may be imposed if specific provisions of the contract/s are violated.
Co-payments - These are user charges or fees levied for consultations with health professionals, medical or investigative procedures, medicines and other supplies, and for laboratory tests. They include charges levied by private health insurance companies to insured persons which must be paid directly through out-of-pocket payments to providers at the time they use health services because these costs are not covered by their specific benefit option.
Fee-for-Service Reimbursement - Fee-for-Service reimbursement is an approach to the payment of healthcare and health services providers based on the number of interventions conducted and/or the number of treatment episodes between a patient and a provider. This type of reimbursement mechanism has been shown to be responsible for cost escalation and patient over-servicing in many contexts.
Financial Risk Protection - The provision of adequate financial protection to all households from catastrophic health-related expenditures. This will ensure that they do not suffer financial hardship and/or are not deterred from using needed health services. This involves minimising or eliminating the barriers that households face when accessing health services, such as the requirement to pay for needed care on the spot.
Health Benefits - This refers to the scope of health entitlements that are offered as part of the package of health services that everyone in a particular population is entitled to. In universal coverage health systems, these usually involve a mix of health promotion, prevention, curative and rehabilitation care. In some instances, this is referred to as the package/s of care.
Health Quality Assurance - This refers to mechanisms that are put in place by a relevant institution or a combination of institutions to monitor and evaluate the compliance of healthcare and health services providers to stipulated quality norms and standards. Within the South African health system this will be done by the proposed Office of Health Standards Compliance.
Health Quality Improvement - This refers to systems, processes and interventions that are implemented across all levels of the health system to progressively and sustainably enhance the quality of healthcare services that are rendered to the national population.
Health System - The combination of organisations, institutions and individuals that are directly and indirectly involved in the provision and delivery of health services to the national population. This includes public, private (for-profit, not-for-profit) as well as non-government organisations.
Mandatory Contribution - This is a compulsory amount of money that an individual or household is expected to make towards the financing of the health system. The mandatory contribution amount is usually expressed as a proportion of a household‟s or individual‟s income or earnings and is collected by a defined government agency as dedicated revenue allocated into the pooled pot of funds.
National Health Insurance - An approach to health system financing that is structured to ensure universal access to a defined, comprehensive package of health services for all citizens, irrespective of their social, economic and/or any other consideration that affects their status.
Pooling of Funds - A process of collecting and combining mobilised financial resources so as to spread the health-related financial risks across a wider pool. It involves the accumulation and management of financial resources to ensure that the financial risk of having to pay for health care is shared by all members of the pool. In universal health systems, risk-pooling or pooling of funds is occurs where payments for healthcare are made in advance of an illness, these payments are pooled in some way and used to fund health services for everyone who is covered - treatment and rehabilitation for the sick and disabled, and prevention and promotion for everyone. The pooled funds can be either from direct tax revenues or a combination of some sort i.e. direct tax allocations supplemented by mandatory, payroll-related contributions.
Population Coverage - This refers to the proportion of the national population that has access to effective universal coverage and financial risk protection. The higher this proportion is, the better the level of financial risk protection and access to needed health services a given population or sub-population group has.
Primary Health Care - The provision of health promotion, preventive, curative and rehabilitative care as close to the household and community as is possible. This approach to health services provision and delivery is based on the recognition that the promotion and protection of health is essential to human welfare and sustained economic and social development. Therefore, health care and health services are rendered in a manner that integrally takes into account the circumstances in which people live, work and interact.
Purchasing - This refers to the systems and processes that government puts into place to create mechanisms for paying for health services that are delivered to the population. Purchasing includes appropriate institutions and organisations making decisions about what services should be provided to a given population and how these services should be funded.
Revenue Collection - This refers to the manner in which financial resources are mobilised or raised to pay for health system costs. Financial resources can be collected through general or specific taxation; compulsory or voluntary health insurance contributions; co-payments such as user fees; and donations from bilateral and multilateral institutions.
Risk-adjusted Capitation - This is a provider payment mechanism whereby healthcare providers are paid a predetermined fee to cover all the health needs of each person registered with them. The fee paid is usually adjusted to take into account of the patient profiles of each provider. The common adjusters include patient gender, age and epidemiological profile. This mechanism is commonly used to pay primary care providers or facilities for their services.
Social Solidarity - refers to building financial risk protection for the whole population through equitable and sustained health financing mechanisms that ensure sufficient cross-subsidisation between the rich and the poor, and the healthy and sick. It is linked to the concept of social justice which puts a limit to how much inequality is acceptable. Such a system allows for the spreading of health costs over a person's lifecycle: paying contributions when one is young and healthy and drawing on them in the event of illness later in life.
Universal Coverage - The progressive development of the health system, including its financing mechanisms, into one that ensures that everyone has access to quality, needed health services and where everyone is accorded protection from financial hardships linked to accessing these health services. This does not imply that the State must provide everything and anything to the population. Instead, it implies that everyone must be given an equitable and timely opportunity to access needed health services, which must include an appropriate mix of promotion, prevention, curative and rehabilitation care. The World Health Organisation defines a universal health system as one that provides all citizens with adequate health care at an affordable cost.
FOOTNOTES:
[1] CMS: Council for Medical Schemes is a statutory body with regulatory oversight for the medical scheme's industry. It is established by an Act of Parliament, the Medical Schemes Act, 1998
[2] Commercialism - This is a business practice that turns goods and services into products for the sole purpose of generating profits ]
[3] Hospi-centric - a health system where the majority of health problems are dealt with at hospital level when patients already present with serious complications
[4] Quadruple Burden of Disease: Refers to HIV/AIDS and TB; Maternal and Child death; Non-Communicable diseases and Violence and Injuries
5 Maternal Mortality Ratio - This is the number of women who die due to pregnancy related causes and is measured per 100,000 live births in a given population. It includes any pregnancy related death and is measured from the beginning of pregnancy to six weeks after birth or termination of pregnancy.
6 Peri-Natal Mortality Rate - Peri-natal mortality is the death of a baby who was born live after 20 weeks of pregnancy or dies within 7completed days after birth measured per 1000 births. It includes stillbirths.
7 Neonatal Mortality Rate - refers to the death of a live born baby within 28 days of birth and is measured per 1,000 live births.
8 Gross Domestic Product (GDP) - This is the market value of all final products (goods and services) produced in a country within a given period, usually a financial year.
9 Catastrophic health expenditure - health care expenditure resulting from severe illness/ injury that usually requires prolonged hospitalisation and involves high costs for hospitals, doctors and medicines leading to impoverishment or total financial collapse of the household.
10 Risk Equalisation - This is a mechanism that is applied to equalise the risk profiles of separate insurance pools in order to avoid loading premiums on the insured members based on some pre-determined health factors
11 Barriers may be regulatory, cultural, geographic and administrative. This should be understood within available resources in the country.
12 National Treasury (2010) Economic Impacts of the National Health Insurance. Draft.
13 The channelling of a patient to another level of care, either a higher or lower level for continuity of care. It is a process in which the treating health practitioner at a particular level of health service channels a patient to a different level of care.
Click here to sign up to receive our free daily headline email newsletter
